
Photo illustration by Slate. Photo by Getty Images Plus.
Two emergency physicians, based at two different hospitals in the New York metropolitan area, are logging their days for Slate. At the end of each shift, they write a response to three questions: What was today like? How did it compare with yesterday? And how do you feel? We have offered them anonymity so that they can write freely about their experiences. Dr. Kelly Keene and Dr. Lauren Serino are pseudonyms. Read Week 1 here, Week 2 here, and Week 3 here.
Dr. Keene, April 14I’m not Jewish, but we had a Passover Seder with my boyfriend’s family over Zoom after my ER shift today. This was preceded by us watching the Rugrats Passover episode, both for a bit of lighthearted comic relief as well as for a quick refresher on the Ten Plagues. I am struck by how eerily some current events are mirroring some of the Ten Plagues: first, the snow turned red as blood at the North and South Poles, then the hail in upstate New York, the swarms of Locusts in Africa, etc. Is this coronavirus but a form of “pestilence,” or is it causing the “darkness” in this modern day plague?
Having trained in an intense ER residency, I’m used to seeing all sorts of critical situations. I’ve delivered babies in the ER parking lot; I’ve seen horrific trauma in which the entire inside of human anatomy was visible; I regularly deal with strokes, sepsis, heart attacks, broken bones, head bleeds, failing organ transplants, etc. I’m used to handling acutely psychotic patients, severely demented patients, drunks, drug addicts; I have often been yelled at, cursed at, spit at, even hit and kicked. Yet nothing has compared to what we are seeing now with Covid. For the first time in my life, going to work scares me, and coming home from work scares me even more—because of the concern that I might bring the infection home to my boyfriend. More and more colleagues (nurses, PAs, attending physicians, residents) are falling sick. Two young residents in NYC reportedly died from the coronavirus.
I can only imagine how this is affecting the residents across the country, the ones who are just starting out in hospitals, and are there to learn the ropes. Some have already been infected, others have sent their spouses and children away to avoid infecting them. They have all been working exhausting 12-hour back-to-back shifts, and the usual venues of decompression (e.g. bars, restaurants, movie theatres, friendly get-togethers) have all been shut down. But beyond the devastating effects on their psyche, it has been detrimental to their education, too. This is supposed to be a time of training and learning, of honing their craft. But the chain of command has been upended by this: Medical students are being graduated early to start pitching in, residents are now acting as work horses, and fellows have had their fellowships discontinued and asked to work as attendings. I worry about their well-being, yes, but I also worry about the future of the U.S. medical landscape as we practice “war time medicine.”
Speaking of “war time medicine”…I’ve been reading the many articles and commentaries calling the ER and hospitals a “war zone” and referring to health care staff as “heroes of the Covid war.” I find the war metaphor both apropos and vexing. The number of projected Covid-related deaths, even with social distancing, is still projected to be between 100,000-240,000. By comparison, about 60,000 were killed on the battlefield in the Vietnam War. Navy ships have been deployed and army field hospitals have been mobilized in multiple regions of the country. The hospital wards are filled with patients lined up on vents, not even a curtain between them for lack of space. There are refrigerated trucks parked outside hospitals serving as temporary morgues holding piles of dead bodies. It looks like a “war.”
If I had wanted to be in the military, I could have had my medical school paid for by the government.
But it is vexing to hear health care workers being compared to military personnel. Yes, we signed up to be front-line staff in treating illness and injuries. We did not sign up to be in combat, we did not sign up to go into “battle” against Covid without proper personal protective equipment, and we certainly did not sign up for endangering our loved ones. If I had wanted to be in the military, I could have had my medical school paid for by the government. Instead, I, along with many other physicians, chose to go hundreds of thousands of dollars in debt to go to medical school and sacrifice a decade of my life to train to be a civilian physician. Let me be clear: Soldiers are not sent to war without necessary equipment, firefighters do not rush into burning buildings without respirators. Why is this lack of PPE acceptable for the health care profession?
The health care system in the United States has been faulty for a long time. Front-line staff in hospitals have been asking for updated equipment for years. Instead, often our profit-driven system focused on improving Press-Ganey (customer satisfaction) scores rather than upgrading supplies that would actually enable better health care. Will this Covid pandemic finally highlight the problems and help drive a proper response from the health care systems and the government? Or will it all fade away in short memory, with our dead colleagues counted as “fallen heroes” and collateral damage from the Covid “war”?
Don’t get me wrong, I am proud to work alongside my ER family, and it is nice to be considered heroic. But that is not how I think of myself. I hope people realize that this is the job we have always done—we have always been frontline staff, treating the sick and injured, serving as the safety net for marginalized populations. I am heartened by the many reports of people coming together all over the world to help each other in this time of crisis. I just hope this moment lasts longer than the pandemic itself.
Dr. Serino, April 15:I woke up to three boxes on my doorstep filled with face shields and a text from NYCPPE saying that our GoFundMe money is stretching even farther, and to expect another delivery of 500 n95’s this week. New York is starting to get what passes as a modicum of control over new COVID cases, but the long haul has only just started. Slightly less contagion is still vastly too much, and the supplies will have to stretch.
The newspaper reports a plateauing death toll, the accompanying graphic is that familiar stretched curve. I drink my still-terrible coffee, a reminder that I’ll never have the option to quit medicine and become a barista. I’ve been waking up to headlines about mortality and economic devastation caused by coronavirus for over a month now, and it has started to feel mundane. I was already refilling my mug when I realized that my anxiety was absent, replaced by a sense of routine. What is the epidemiological equivalent of the banality of evil? Maybe, the prosaicism of pathology. I finished my breakfast, checked the mail, bleached the door handle, and watched a COVID treatment panel discussion about the utility of blood thinners in the acute phase of disease, all things that are starting to seem like second nature now.
What is the epidemiological equivalent of the banality of evil? Maybe, the prosaicism of pathology.
On the panel, a few doctors from New York were discussing what they’ve been seeing in terms of clinical picture and treatments that are working—or not. Two of the doctors described scenes that told very different stories. One told the story I have been watching unfold—ER’s crowded to the point of collapse, a crushing number of deaths, the shocking acuity and multi-organ-system derangement in even the younger patients. But the other spoke of an experience more in line with the overall data—yes, far too many young in the ICU, but the elderly and comorbid older patients making up the bulk of the dying; the hospital strained, but able to keep up.
ProPublica has an interactive zip code map that updates daily with the number of cases in each NYC area. The first doctor worked in an area with 71 percent greater number of infections than the city average. The other? In an area with 60 percent less than the average. Even in the pandemic epicenter, eight miles made a vast difference.
Poverty is a terminal illness in itself, and it’s why the hardest hit neighborhoods, in the hospitals where I’ve spent my career, report the highest piles of bodies. Bodies who had insufficient access to preventative medical care, healthy diets, and too many people squeezed into a tiny apartment. COVID can kill you no matter how much money you have. But not having it correlates closely with the risk factors that make it much more likely to kill you and the people you love.
Short of a vaccine, there’s no way to immediately solve this entrenched problem just by recognizing it’s there. But that doesn’t make it any less important to acknowledge and, maybe, to remember—if we are wise enough to learn from some of our myriad mistakes during the pandemic. The virus, more than anything, reminds us that the world is interconnected. None of us are separate. And devastation in one community is not only their loss, but may set off a chain of contagion that affects people more broadly, whether that’s a few miles or a continent away.
Before bed, I called a friend who wanted to congratulate me on the slowing of NYC deaths. I assured her it wasn’t all my doing, but thanks. She laughed. She has an innate optimism I’ve always been jealous of.
“This too shall pass,” I said, but it sounded dismissive and, more than that, untrue. Sometimes, the ghost of an experience sticks around simply because it enjoys the haunt. I wonder if COVID will be that way: One of my colleagues said she’s going to take the next two weeks recovering from the last two weeks, and then repeat the process for the foreseeable future. Maybe, instead of passing, the realists’ alternative is, “This too shall become normal.”
Today was hard. I keep looking for a more evocative adjective but I just keep coming back to this: Today was hard. I turned in my badge at the hospital that I’ve worked at for the last five years. There has been mounting violence in the ER and not enough done to protect its workers. Things had become dangerous there, long before the presence of the virus. In a few days I start at a new hospital. There will be some familiar faces there. Still, it’s hard.
Dr. Keene, April 15:A 73-year-old male patient is rushed in, his oxygen saturating reading 56 percent (normal is over 95 percent). He is visibly in respiratory distress, breathing shallowly and rapidly, able only to eke out one word at a time. We place a non-rebreather mask on him to give him maximal oxygen, but his saturation only improves to about 85 percent. Knowing time is limited, I had to ascertain his “code status,” specifically, whether he would want to be placed on a ventilator when he could no longer support his own breathing. He made it clear between labored breaths that intubation was something he would never want, understanding that he would die the minute he tired out from his puffing and panting. He told me of his wife of 45 years, now home alone, unable to be by his side because of the no-visitor rule that most NYC hospitals have instituted.
We have one iPad in the ER to allow patients to facetime with their loved ones, but it is currently being used in the next room by a 56-year-old man, also critically ill from Covid, telling his children in Chicago he loves them before being induced into a medical coma for intubation. I pull out my cell phone and helped my patient Facetime his wife. I hold back tears as they exchanged what might be their last loving words to each other. Overhead on the PA system, I hear more calls of “rapid responses” for admitted patients who are decompensating on the hospital wards, and then upgrades to “code blue,” for patients who are dying on the wards—dying so utterly alone, with no one to hold their hand. Death has always been a sad part of my job, but now we are the ones saying goodbye for the patients. Having to do so remotely, over a phone or tablet, seems that much worse.
Dr. Serino, April 16:Hairdressers have a mafia, of which I knew next to nothing prior to the pandemic, and which I’m intensely grateful to know now. Their magic is how, over the course of an hour, five hundred dollars could be amassed, and, three days later, 5 gallons of barbicide and boxes upon boxes of gloves appeared at my doorstep—just in time to add them to my next PPE deliveries tomorrow night. Disinfectant online is still almost universally sold out. But, no worries, they know a guy.
Meanwhile, friends who have never cooked a day in their life have become master bread bakers. The clumsiest amongst us has taken a daily ballet class, and isn’t half bad. Some are learning to program or play the guitar.
There have been a lot of unexpected things happening during the pandemic. But none have amused me more than this: My friends keep calling me for medical advice. This in itself isn’t uncommon. Strangers will try showing me their rashes at dinner parties when they find out what I do. But this time, it’s couples who don’t live together, each member contacting me separately, and all with the same question:
When can we have sex again?
I’m almost positive, based on the conversation, that neither knows the other is calling to ask. It’s romantic, really. Couples, isolated in different apartments, perhaps one or both sick, so concerned for the other’s welfare above their own animal needs that they aren’t willing to risk it without medical clearance.
Somehow, on my days out of the hospital, I have become the Dr. Ruth of Coronavirus.
And today, when the first of the couples who called me reached back out, each barely an hour apart—he to announce that he is now asymptomatic going on three weeks after being sick with COVID, and she to say she remained perfectly healthy and her roommate had chosen to move out and isolate back home—I was finally able to give someone medical advice they actually wanted to hear.
Dr. Serino, April 17:My contract at my new position was cancelled today. The position—one requiring procedural experience, best filled by a critical care doc, i.e., an intensivist or someone like me—is now going to be filled by hospitalists: doctors who only work on the hospital floor and don’t have the procedural training I do. Apparently the people hiring think this can be taught in a pinch, and that other docs, possibly from specialties that don’t usually do floor medicine, can take over for those hospitalists if needed.
Another contract—this one for per diem assistance in a busy system—was supposed to start placing me on shifts to help during the peak of our crisis. The company offering me that contract told me to be prepared to start three days after I was hired, and then it never called. Another doc was also waiting for that same call. It never came.
Since the start of the pandemic, NYC has been asking doctors from other places to come help and fight the COVID crisis. It was akin to a call to arms during a war: Do you have or did you have a medical degree in any state? Are you able-bodied enough, even if you are sick or old? Are you willing to be a hero on the front lines? There’s honor to be won in a war, son, do your part.
Health care workers from all over the country were directed to a NYC department of health online portal for assistance with placement, so that doctors could be matched with the hospitals that needed them most.
I’ve spent my career in NYC. I was prepared to jump in, so I reached out directly to the places that I knew were being hit hard to see if I could offer my services, foregoing the delays inherent in a bureaucratic government website. Friends, doctors I’d trained with, doctors already living and working throughout the city who wanted to be of broader use, did the same. All of us were already familiar, in a way those out-of-towners were not, with what a 12-hour shift in a COVID-saturated urban ER was like.
But the hospitals seemed strangely uninterested; their rhetoric didn’t match their actions—it was hard to get in contact with anyone. Getting in touch with someone at the VA took five calls, three emails, a week, and then finally I received the internal e-mail address of the physician recruitment team. That address bounced back. Hospitals took my CV, my phone number, then never followed up. During this time, I received calls from recruiters—middlemen hired at a high premium by hospitals during staffing shortages—promising jobs at some of these same hospitals. Companies who took my CV, said they had immediate need, and then, again, went silent. Friends and colleagues mentioned they were in the same situation, even though we were in the thick of the patient crush.
Strange.
Days passed. Finally, two hospitals said they would start the credentialing process and would need us to start immediately. We opened our schedules. Committed and then…
Crickets.
As this was happening, volunteers were placed through the city DOH website. Many physicians I spoke with directly, some retired with medical conditions in high-risk age groups, were volunteering to do what seemed to be the necessary thing and return to work, and many were placed—without pay, in overcrowded ERs, without adequate PPE. Not shockingly, some began to get ill. Already, some health care workers had died.
Meanwhile, other doctor friends and I kept trying to work. We kept wondering, too, why weren’t we being hired?
Hospitals were willing to pay premiums in some situations: they offered large hourly rates to out-of-state physicians who were being asked to come live in hotels and be deployed wherever they were needed each day, to work 13-hour days, 14 days in a row without a day off, in physically and emotionally strenuous environments. Premiums one anonymous administrator told me they prefer to pay because offering hazard pay to local per-diem physicians sets a bad precedent, and wages are sticky. It’s harder to reverse a temporary increase in rate or decrease the number of shifts for local new per-diems than it is to just spend more on doctors who will get on a plane and quietly leave at the end of their tenure. I rarely see the ER staffing agencies hospitals use to execute these callous strategies mentioned in news stories. They’re an invisible part of the system.
There’s nothing like a pandemic to bring out the opportunists.
Most of us have been OK with living our lives as if taking care of others is more important than taking care of ourselves. Hospitals exploit this feeling.
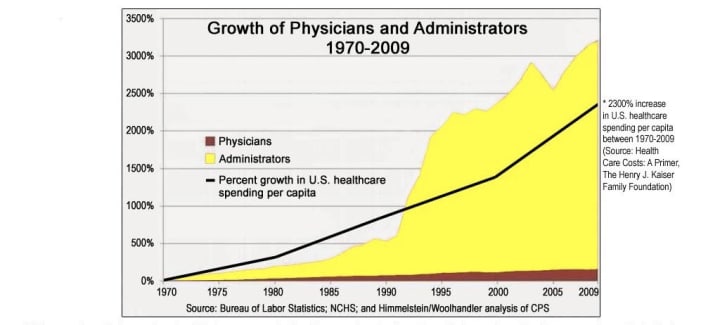
Doctors learn the business of the body, not the business of medicine. But modern health care is an industry with a bottom line measured in dollars, not wellness. As we train, we’re told to “stay in our lane”—an important lane, to be sure—and just worry about being good healers. The rest, the pesky business of how the wheel turns, can be managed by the rapidly expanding pool of administrators. In “staying in our lane,” we don’t feel the insidious ways the business of medicine has eroded the value of the doctor-patient relationship. Instead, patients have become a commodity and physicians a cog. We’re blind to the chaos and danger around us. We might note how focused administrators are on metrics of efficiency and patient satisfaction scores, even if efficiency doesn’t mean quality, and higher patient satisfaction scores are linked to higher overall mortality rate. But we’re hired to provide the services approved by the hospital, and insurers, which is frequently not to our own standards of patient care.
{kind=link}
Doctors learn the business of the body, not the business of medicine. But modern health care is an industry with a bottom line measured in dollars, not wellness.
I see this dynamic continuing in the midst of the COVID crisis. As hospitals and politicians continue calling for help in public, the rhetoric has been that there are too few doctors to manage the crisis. They said this even as doctors were fired or told to leave mid-shift for wearing their own protective equipment. Colleagues who were pointing out dangerous practices for both employees and patients were asked or pressured into leaving. Colleagues who were lower risk and looking for fairly paid work were passed over because other health care workers—who were made to believe there were no other doctors available to work—were being brought in as unpaid labor. They were told there was no money to be found, despite high reported revenues and administrative salaries in the multi-millions.
In writing this I wondered if this is the time to talk about how the business of health care is affecting us, as hospitals proclaim extreme need while not hiring available doctors. But there is no way to separate the business from the care anymore. We’re no longer given the luxury of that separation, because it is the business and the bottom line that has created this situation where the sacrifice of health care lives is considered inevitable.
Even as our sense of purpose is being preyed upon, we‘re afraid we’ll be seen as selfish if we ask for reasonable compensation, even as administrative bloat continues to increase, and insurers continue to collect their premiums. We worry that society sees us as greedy opportunists, even as we must practice medicine in unsafe conditions, at the whims of insurers and hospital authorities who profit from our sense of obligation and decide how we provide care, and then sends us out to be the messenger, placing us between the patients and their policies. We know how much everyone loves the messenger.
It seems that I have inadvertently become the messenger. So here is my message: If hospital systems really cared about health—of their workers, their patients, their communities—they have been extremely good at hiding it from me and all the physicians who have been looking to work within their walls.
The language of war, or sacrifice, is used when you want to mentally prepare people for a certain amount of unavoidable front-line losses. The system leverages our sense of moral obligation to exploit us.
Dr. Keene, April 17A robust 72-year-old man is sitting up on the stretcher, talking on the phone with his family member about having to be admitted for his new onset atrial fibrillation, an irregular heart rhythm. During his 3.5 hour ER stay, I saw the cardiology team come by his side four times, checking to see if a medication has successfully converted his rhythm back to normal. I look at my resident in disbelief—neither of us had ever seen cardiology swing by to see a stable patient in the ER so frequently.
Another man comes in requesting a urinary suprapubic catheter change, a fairly simple and quick procedure. But he demands that a urologist perform the exchange and refuses to let ER staff touch it. Apologetically, I explain the situation on the phone with the urology consultant and he replies, “No problem, I’ll come and take care of you. I’m sure you guys have your hands full in the ER.”
Next comes a 40-year-old female who returns to the emergency room for a repeat beta-HCG level, a pregnancy hormone we need to recheck because she might be having an ectopic pregnancy. Because she was seen by our OB/Gyn team a couple days prior, I call the OB/Gyn consult just to touch base, mostly to ensure the patient has follow up. To my surprise, the consultant comes by the ER to see the patient, even though I told her it was not necessary. Again, my resident and I exchange a look—our consultants have all been exceptionally nice and helpful during this whole time of Covid crisis.
Largely, I attribute this “niceness” to medical professionals coming together in solidarity, supporting each other in this pandemic. Across the country, many subspecialty health care providers (cardiology, gastroenterology, etc.) have been recruited to the ERs and to the inpatient units to assist with the influx of Covid patients. The rest of them, who have been experiencing a lower volume than usual, have been trying to pitch in any way they can. It is incredibly touching to feel the support of colleagues, to know we are there for each other, even if we may often have disagreements in normal times (e.g. surgical services often “punting” patients to medicine rather than admitting them to their own service).
But on a lighter note, I also think I’ve been seeing consultants in the ER more frequently partly because they are bored, and partly because they are just excited to see patients with diseases that are non-Covid related.
Dr. Serino, April 18:During a telemedicine consult this morning, my patient seemed apologetic and uncomfortable, as if he was speaking through gritted teeth.
“I’m having terrible abdominal pain,” he said.
“When did it start?”
“A week ago.”
He described severe, acutely worsening lower abdominal pain, the inability to have a bowel movement for over five days, and a history of obstruction. He was vomiting. It didn’t look right, like dark, wet coffee grounds. Every tiny movement to his trunk felt like knives in his abdomen. “I’m getting lightheaded,” he said, quietly, as if he was confessing a secret. The tenor of his voice revealed that he knew this wasn’t going to be solved with a phone call.
“Sir, you…”
He cuts me off. “I really don’t want to go to the hospital”
“You have to.”
“I don’t want to get the virus.” He sounds like he’s about to cry.
I think about the tally of COVID deaths being recently adjusted for presumed cases found deceased at home. I wonder how many all-causes of death are increasing because the fear of COVID outweighs the fear of their current illness. In fairness, the fear of COVID is the fear of dying alone, without your family, shrouded in wires. I get it.
We complain about the frustrations caused by patients who show up in the middle of a busy shift complaining of two years of back pain, or requesting a pregnancy test, or with a bug bite. But when the volume of non-covid patients dropped precipitously, we knew the worried well didn’t make up that large of our patient population.
There are still appendicitis, heart attacks, and strokes happening in the community. There are broken bones, bleeding in pregnancy, and kidney stones. We have been asking where our patients went, but we know where they went. Or rather, where they didn’t go. They remain the most adherent to the stay-at-home orders. They are delaying or foregoing care, simmering in their otherwise-treatable pathologies at home.
Finally, finally, I was able to convince him to go. He put on a fabric mask and a pair of ski goggles and let me call the ambulance because he was too weak to drive. I couldn’t promise him that he wouldn’t catch COVID in the ER. The opposite—I’m worried that he will, and will be at increased risk of death because of his comorbidities. But while COVID might kill him, without treatment his obstruction, internal bleeding and infection certainly will.
I feel like there are only bad and less-bad options when it comes to managing health care right now, even as we fall back from the initial surge of cases.
I feel like there are only bad and less-bad options when it comes to managing health care right now, even as we fall back from the initial surge of cases. I have to consider my advice carefully, leveraging as many outpatient and telemedicine treatment options as I safely can—which is vastly more than I have ever used before. The number of people whose chronic and acute medical conditions will make it worse for them should they catch COVID are, of course, the same people whose conditions will be worsened by trying not to. COVID is a chameleon, constantly presenting in new and wildly varied ways. I wish we had planned for the ways it might kill a person without them ever catching it at all.
Dr. Serino, April 19:This afternoon I went to a party on Zoom hosted by a group out of London called the Co-Reality collective. It was large —hundreds of people, multiple “rooms”—and most people were costumed, friendly, and eager to connect across time and miles. The theme was moon landing, and at midnight their time, we stopped to share a screen. The host cued up a movie that revealed our place in the universe: floating on a small blue dot in a mote of sunlight. This passage from Carl Sagan’s “Pale Blue Dot” was narrated:Our planet is a lonely speck in the great enveloping cosmic dark. In our obscurity, in all this vastness, there is no hint that help will come from elsewhere to save us from ourselves…. To me, it underscores our responsibility to deal more kindly with one another…
Our planet is a lonely speck in the great enveloping cosmic dark. In our obscurity, in all this vastness, there is no hint that help will come from elsewhere to save us from ourselves…. To me, it underscores our responsibility to deal more kindly with one another…
I’ve been struggling with feeling like the distance between where we’re at now in the pandemic timeline, and the light at the end, is as vast as that between earth and sun. But as the movie ended and everyone shared how grateful they are for the support, even the online support of strangers, then got up to have a digital dance party, I realized that what we’re doing isn’t socially distancing at all. It’s only physically distancing.
I stopped by my old hospital tonight to drop off a surprise donation: a plexiglass intubation box meant to decrease COVID exposure during aerosol producing procedures. My favorite senior resident was on the night shift. I’ve known him since he was an intern and I was a relatively new attending. He was having a hard time then, and reminded me of myself when I felt like I didn’t fit into the department my first year of residency. I hoped I could model myself after the attendings who supported me, in some small way, and be a nonjudgmental ear. A safe person to come to.
“Hey, thanks for looking out for us,” he said as I handed over the box.
“No problem.”
“You’ve been really vocal about the stuff that affects us even when we can’t be. It’s appreciated.”
I nodded, hoping he knows that I won’t stop feeling a responsibility towards them even if I’m not there for shifts.
“Oh hey, you also still owe me that bottle of champagne, so maybe don’t forget that next time?”
I laughed.
If a resident does a spinal tap and the lab reports that it has returned without a single drop of blood in it, we call it a champagne tap. It’s a demonstration of the resident’s skill. To congratulate them, you gift a bottle of champagne. It’s supposed to be a reward for the first time they do it, not the hundredth. But, as he reminded me, these are unprecedented times.
“I like Dom, but Veuve will do.”
Dr. Serino, April 20The guy in apartment 1A has a knack for walking by the laundry room in the brief moments just after I have stripped completely naked and am shoving my COVID-contaminated scrubs into the laundry, but before I have covered myself up with a robe. Prior to the pandemic we had only nodded congenially at each other if we passed the mailbox. Now we just sidestep one another and keep moving.
I was outside tonight, in the middle of the large complex of apartment buildings where I live, when the clapping started. I’ve heard it some days at 7 p.m. when I’m not at work, but today was the first time I wasn’t inside from the vantage of my own room. I looked up and saw as windows burst open and bodies leaned out, clanging pots and pans, yelling thank you. The shouting is ostensibly for the health care workers, yes, but also for one another. I can feel how badly those bodies want to burst out of their apartments like the cherry blossoms on the branches of the trees in Prospect Park.
Dr. Serino, April 21Even as the number of overall cases is decreasing, there are still mounting number of colleagues and friends becoming ill. As time goes on, we are losing our degrees of separation between someone who has died or is critical.
My mom said on the phone today that she and my dad are going stir crazy. “I feel like we will never see you again!” She said it in a jesting tone, but I know she means it. They live across the country. They’re scared. They’re worried about me. I also wonder how long it’s going to be. It’s been on my mind since my friend’s mother passed away from COVID a few days ago. He can’t go to the funeral. But worse, so much worse, he wasn’t able to go hold her hand in the hospital as he knew she was dying. Forget the memorial, it’s what he couldn’t do for her while she was alive that guts him—and so many in his situation—now. I wish I could say I can’t imagine that scenario, but I can, and it makes me wonder, not just when I will see my parents again, but what I will have to do to make visiting an 85- and 73-year-old safe.
The goal of curve-flattening was to give the health care system a chance to prepare. There was no way that we would have a vaccine by now, but I’d hoped that we would have a better handle on the ever-evolving and truly baffling pathophysiology of virus. Or a medication we could rely on. Even just reliable access to PPE. The goal wasn’t just to decrease the crush of initial patients, which, thank goodness, is starting to work. The problem is, unless our only goal was to delay the inevitable, we have to know what we are replacing lockdown with.
The W.H.O. has outlined six conditions for any government that wants to start lifting restrictions:
1. Disease transmission is under control
2. Health systems are able to “detect, test, isolate and treat every case and trace every contact”
3. Hot spot risks are minimized in vulnerable places, such as nursing homes
4. Schools, workplaces and other essential places have established preventive measures
5. The risk of importing new cases “can be managed”
6. Communities are fully educated, engaged and empowered to live under a new normal
I find most of these infuriatingly vague and it’s hard to imagine implementing #2 successfully in democratic societies. But they make a good point—other than controlling transmission with further lockdown, I don’t see how we have made strides on #2-6. Even #1 could be easily reversed.
I’m anxious for reliable antibody testing to actually be available, since we’ve been hearing rumors of it here in NYC for a while now. I called the DOH today to ask how, as a health care worker, I could get tested, but I’m not optimistic, since the consultant didn’t know any more than I did. I still put my hopes in vaccine challenge trials. Maybe the Plaquenil study I’m in will show positive results. On an “emerging expert” panel I took part in the other day (experts on any novel pathogen being the people who are seeing enough cases that they can say—here are all the weird things that I’m witnessing, here’s what didn’t work, here’s what did) we tried to put together a wish list of practical actions that would fulfill the WHO conditions. Without large-scale national coordination, local behavioral changes will only put out satellite fires. There’s no question that we will move forward somehow. That’s the only direction to go. I just hope that the way forward comes with an actual, specific plan.
Readers like you make our work possible. Help us continue to provide the reporting, commentary and criticism you won’t find anywhere else.
Join Slate Plusfrom Slate Magazine https://ift.tt/2znFQLD
via IFTTT
沒有留言:
張貼留言